Image


▼This medicine is subject to additional monitoring. This will allow quick identification of new safety information. Adverse events should be reported. Reporting forms and information can be found at yellowcard.mhra.gov.uk for the UK and hpra.ie/homepage/about-us/report-an-issue for Republic of Ireland. Adverse events should also be reported to UCB Pharma Ltd at ucbcares.uk@ucb.com or 0800 2793177 for the UK and UCB (Pharma) Ireland Ltd at ucbcares.ie@ucb.com or 1800 930075 for Republic of Ireland.
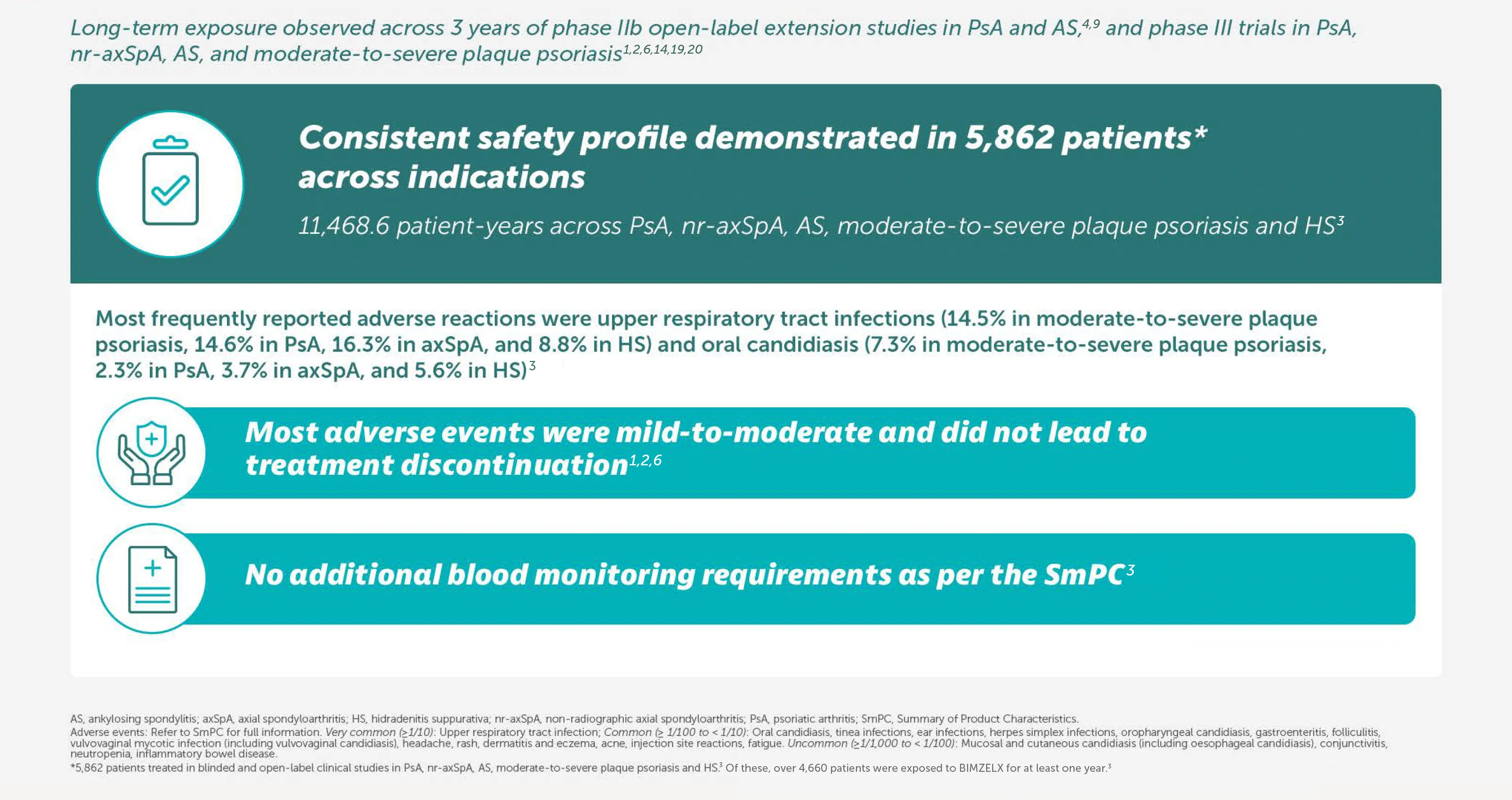
BIMZELX® (bimekizumab) is indicated for the treatment of: active PsA, alone or in combination with methotrexate, in adults who have had an inadequate response or who have been intolerant to one or more DMARDs; active nr-axSpA, in adults with objective signs of inflammation as indicated by elevated CRP and/or MRI, who have responded inadequately or are intolerant to NSAIDs; and active AS, in adults who have responded inadequately or are intolerant to conventional therapy.3
In two pivotal phase III trials, 43.9% (n=189/431) of biologic-naïve and 43.4% (n=116/267) of TNFi-inadequate responder patients achieved the primary endpoint of ACR 50 at Week 16 with BIMZELX (versus 10.0% [n=28/281] and 6.8% [n=9/133] with placebo, respectively; (p<0.0001 and p<0.001 for each trial respectively)1-3
Primary endpoint in both trials: ACR 50 at Week 16 (p<0.0001 vs placebo)1,2
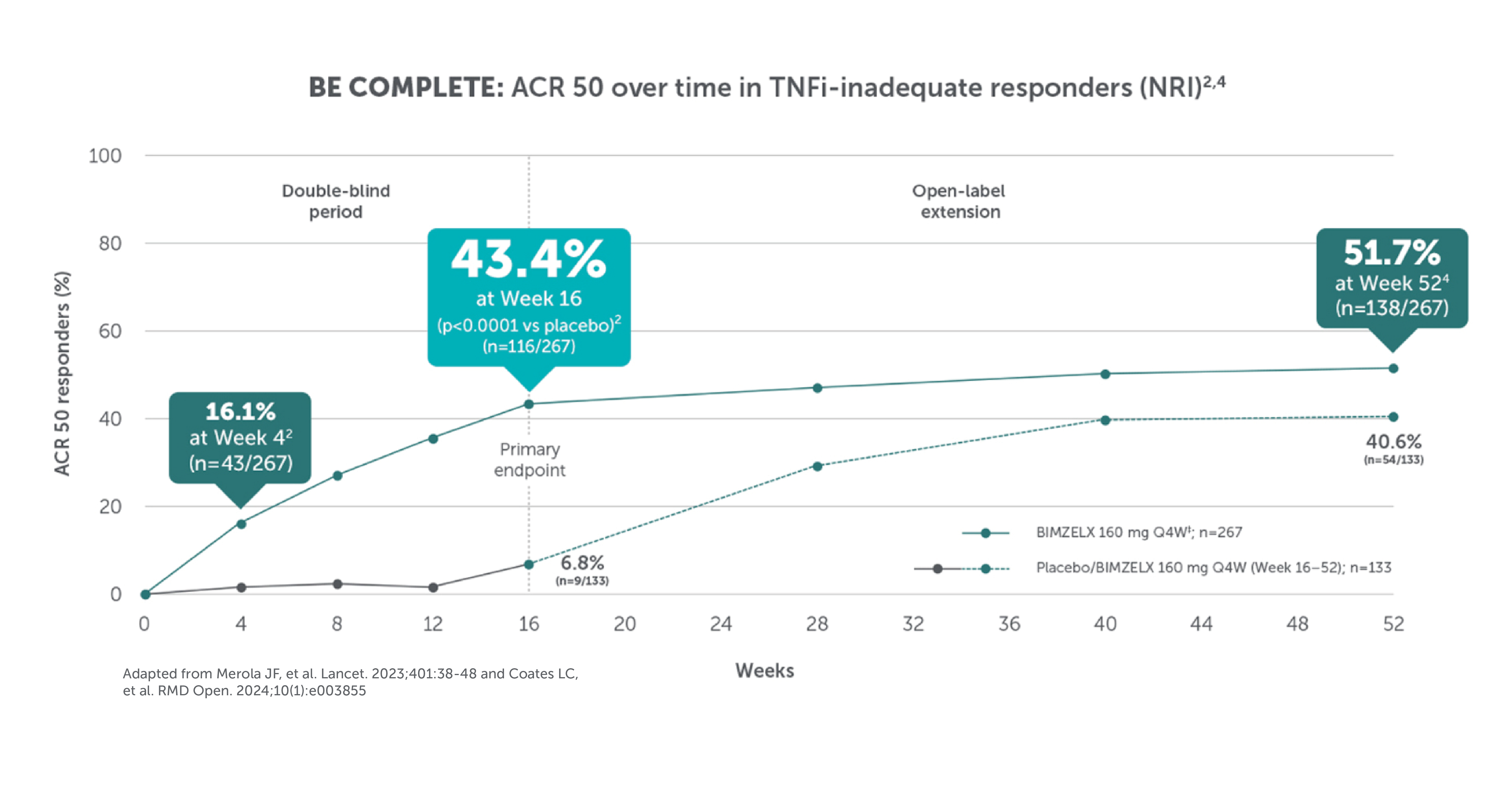
ACR 50 was achieved by 43.9% (189/431) of biologic-naïve and 43.4% (116/267) of TNFi-IR patients with PsA at Week 16 (primary endpoint in BE OPTIMAL and BE COMPLETE),1–3 54.5% (235/431) and 51.7% (138/267) at Week 52 respectively (NRI analysis).4,5 ASAS 40 was achieved by 47.7% (61/128) of nr-axSpA patients and 44.8% (99/221) of AS patients at Week 16, (primary endpoint in BE MOBILE 1/2);6 60.9% (78/128) and 58.4% (129/221) at Week 52, respectively (NRI analysis).3,6 Rapid onset was demonstrated by numerically higher responder rates (ACR 50) observed when compared with placebo at Week 4 in BE OPTIMAL, 17.6% (76/431), versus 3.2% (9/281); and BE COMPLETE, 16.1% (43/267) versus 1.5% (2/133) respectively.1,2 Rapid separation in ASAS 40 response rates was observed within 1–2 weeks after single a dose of BIMZELX versus placebo; 16.4% (21/128) versus 1.6% (2/126) at Week 1 in BE MOBILE 1, and 16.7% (37/221) versus 7.2% (8/111) at Week 2 in BE MOBILE 2 (NRI analysis).7,8 Reduction of patient limitations was demonstrated using MDA in PsA and ASDAS <2.1 in axSpA. MDA was achieved by 45.0% (194/431) of biologic-naïve and 44.2% (118/267) TNFi-IR patients with PsA at Week 16 (NRI analysis).3 ASDAS <2.1 was achieved by 46.1% (59/128) of nr-axSpA patients and 44.8% (99/221) of AS patients at Week 16, BE MOBILE 1 and BE MOBILE 2 respectively (exploratory endpoint, MI analysis).3

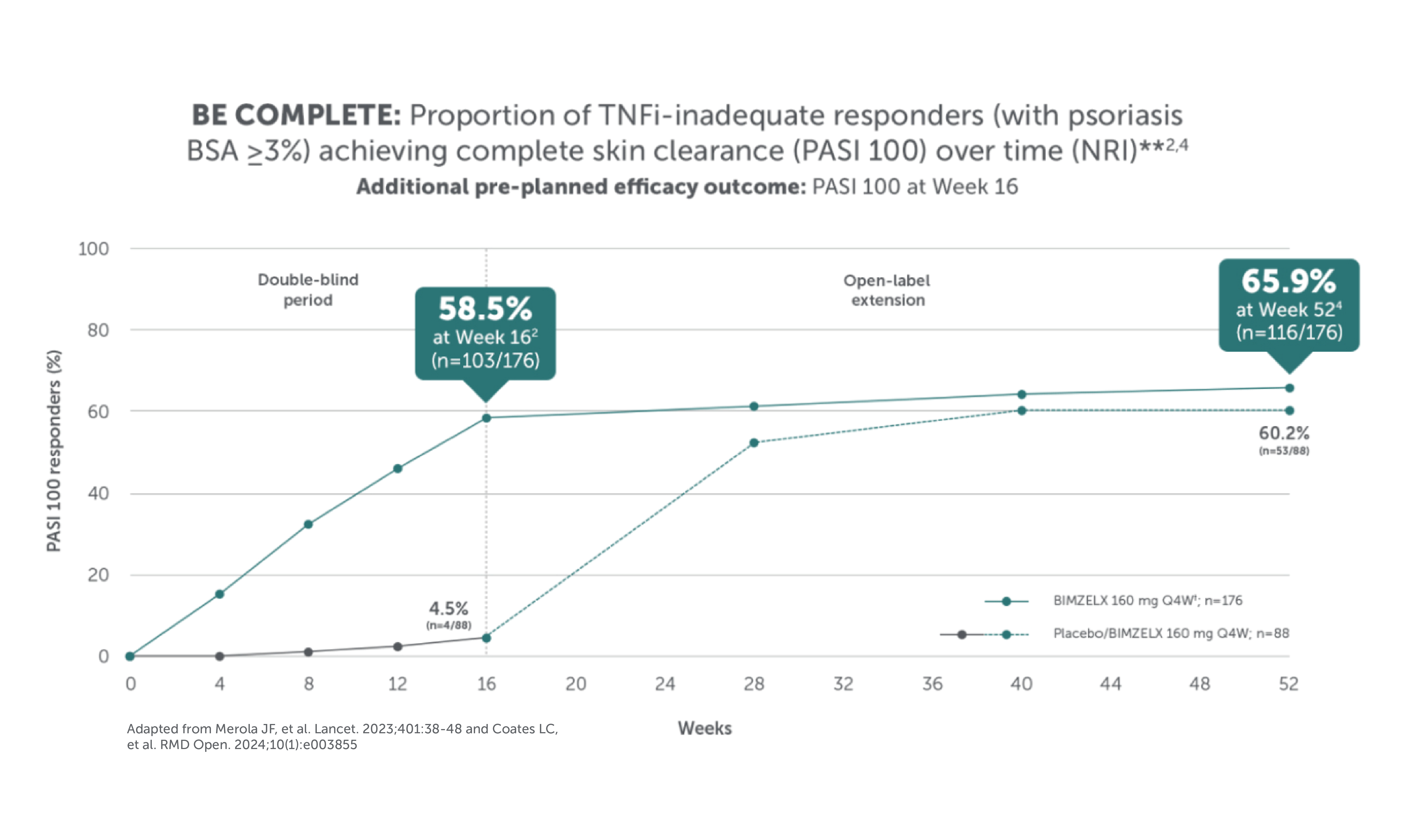
After Week 16, patients in BE OPTIMAL and BE COMPLETE were aware that they were receiving active treatment, which may have affected the results. Week 52 data are for patients who completed the BE COMPLETE phase III trial (which ran for 16 weeks) and then entered the BE VITAL open-label extension study.1,2,4
After Week 16, patients in BE OPTIMAL and BE COMPLETE were aware that they were receiving active treatment, which may have affected the results. Week 52 data are for patients who completed the BE COMPLETE phase III trial (which ran for 16 weeks) and then entered the BE VITAL open-label extension study.1,2,4
*In BE OPTIMAL, ACR 50 was achieved by 17.6% (n=76/431) at Week 4 (vs 3.2% n=9/281 with placebo), 43.9% (n=189/431) at Week 16 (vs 10.0% [n=28/281] with placebo, p<0.0001), and 54.5% (n=235/431) at Week 52 of biologic-naïve patients in the BIMZELX treatment arm (NRI analysis).1,5 In BE COMPLETE, ACR 50 was achieved by 16.1% (n=43/267) at Week 4 (vs 1.5% [n=2/133] with placebo), 43.4%(n=116/267) at Week 16 (vs 6.8% [n=9/133] with placebo, p<0.0001), and 51.7% (n=138/267) at Week 52 of TNFi-IR patients in the BIMZELX treatment arm (NRI analysis);2,4 **90.0% (n=388/431) of patients who completed 16 weeks of treatment remained on BIMZELX at Week 52;5 †In BE OPTIMAL, mean vdHmTSS change from baseline was 0.01 at Week 16 (vs 0.36 with placebo) and 0.08 at Week 52 in the overall population BIMZELX treatment arm (n=365; NRI analysis).,5 ‡BIMZELX is approved for Q4W/Q8W dosing with PsA in coexisting moderate-to-severe plaque psoriasis.3
After Week 16 all patients were aware that they were receiving active treatment, which may have affected the results. Week 52 data are for patients who completed the BE COMPLETE phase III trial (which ran for 16 weeks) and then entered the BE VITAL open-label extension study

After Week 16 all patients were aware that they were receiving active treatment, which may have affected the results. Week 52 data are for patients who completed the BE COMPLETE phase III trial (which ran for 16 weeks) and then entered the BE VITAL open-label extension study.
After Week 16 all patients were aware that they were receiving active treatment, which may have affected the results. Week 52 data are for patients who completed the BE COMPLETE phase III trial (which ran for 16 weeks) and then entered the BE VITAL open-label extension study.
After Week 16 all patients were aware that they were receiving active treatment, which may have affected the results. Week 52 data are for patients who completed the BE COMPLETE phase III trial (which ran for 16 weeks) and then entered the BE VITAL open-label extension study.
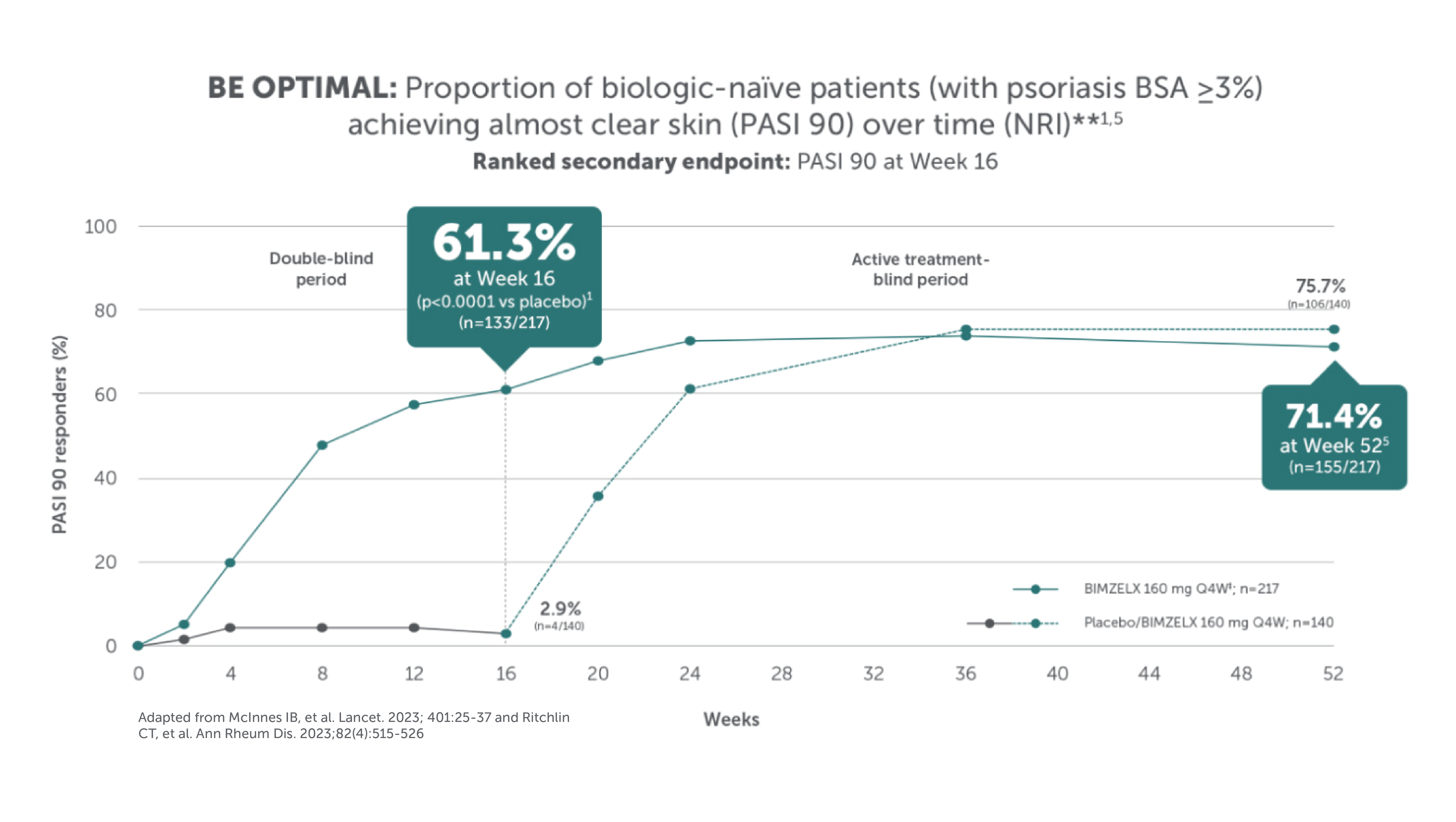
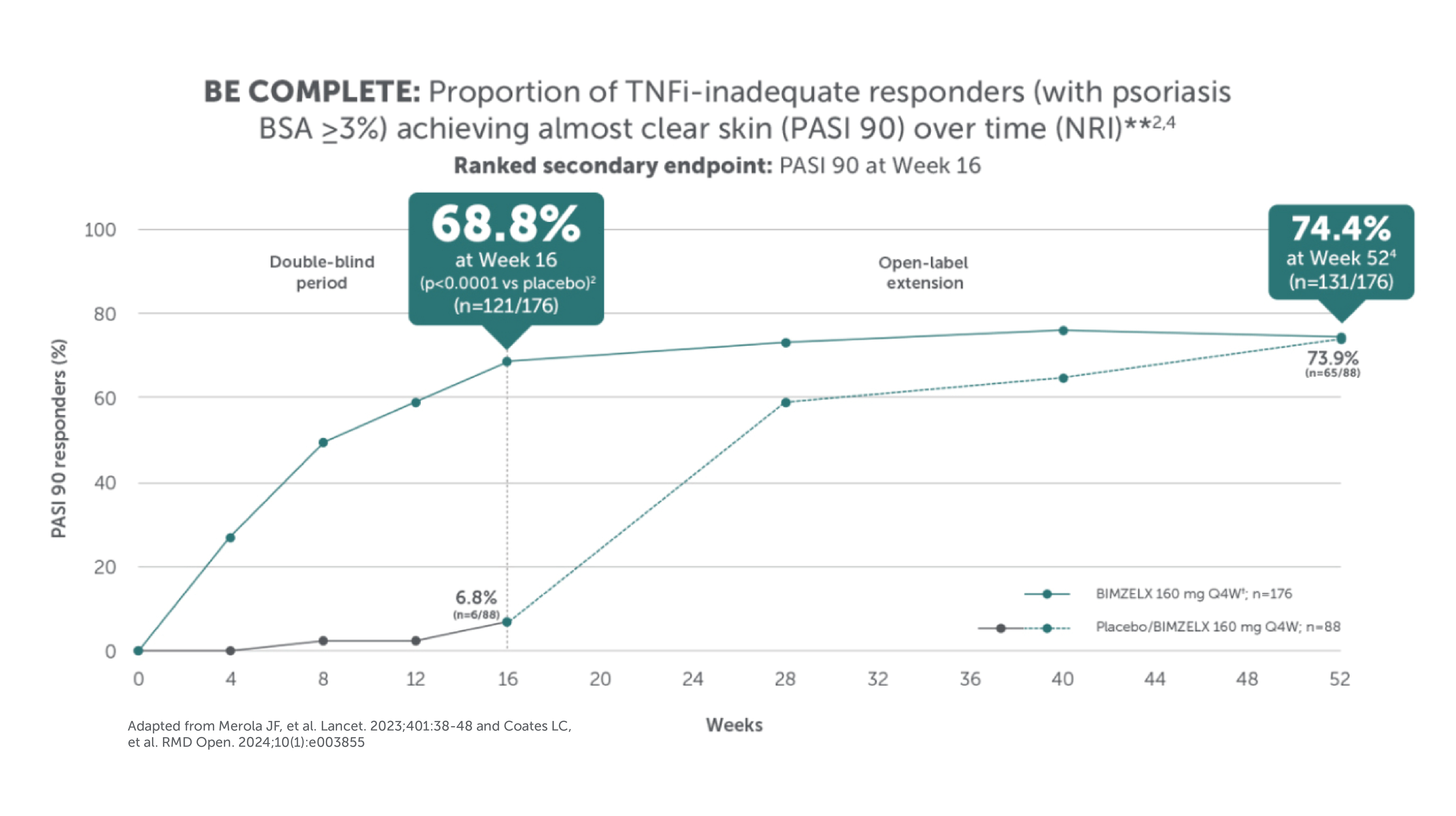
*In BE OPTIMAL at Week 16: PASI 90 was achieved by 61.3% (n=133/217) with BIMZELX and 2.9% (n=4/140) with placebo, and PASI 100 was achieved by 47.5% (n=103/217) with BIMZELX and 2.1% (n=3/140) with placebo; at Week 52: PASI 90 was achieved by 71.4% (n=155/217) and PASI 100 was achieved by 60.8% (n=132/217) of patients in the BIMZELX treatment arm (NRI analysis).1,5 In BE COMPLETE, at Week 16: PASI 90 was achieved by 68.8%% (n=121/176) with BIMZELX and 6.8% (n=6/88) with placebo, and PASI 100 (additional efficacy outcome) was achieved by 58.5% (n=103/176) with BIMZELX and 4.5% (n=4/88) with placebo; at Week 52: PASI 90 was achieved by 74.4% (n=131/176) and PASI 100 was achieved by 65.9% (n=116/176) of patients in the BIMZELX treatment arm (NRI analysis);2,4 **PASI response in patients with psoriasis involving at least 3% BSA at baseline.1,2,4,5 †BIMZELX is approved for Q4W/Q8W dosing with PsA in coexisting moderate-to-severe plaque psoriasis.3
‡ For some patients with plaque psoriasis (including psoriatic arthritis with coexistent moderate to severe psoriasis) and a body weight ≥ 120 kg who did not achieve complete skin clearance at week 16, 320 mg every 4 weeks after week 16 may further improve treatment response.3
After Week 16, patients in BE OPTIMAL and BE COMPLETE were aware that they were receiving active treatment, which may have affected the results. Week 52 data are for patients who completed the BE COMPLETE phase III trial (which ran for 16 weeks) and then entered the BE VITAL open-label extension study.
After Week 16, patients in BE OPTIMAL and BE COMPLETE were aware that they were receiving active treatment, which may have affected the results. Week 52 data are for patients who completed the BE COMPLETE phase III trial (which ran for 16 weeks) and then entered the BE VITAL open-label extension study.
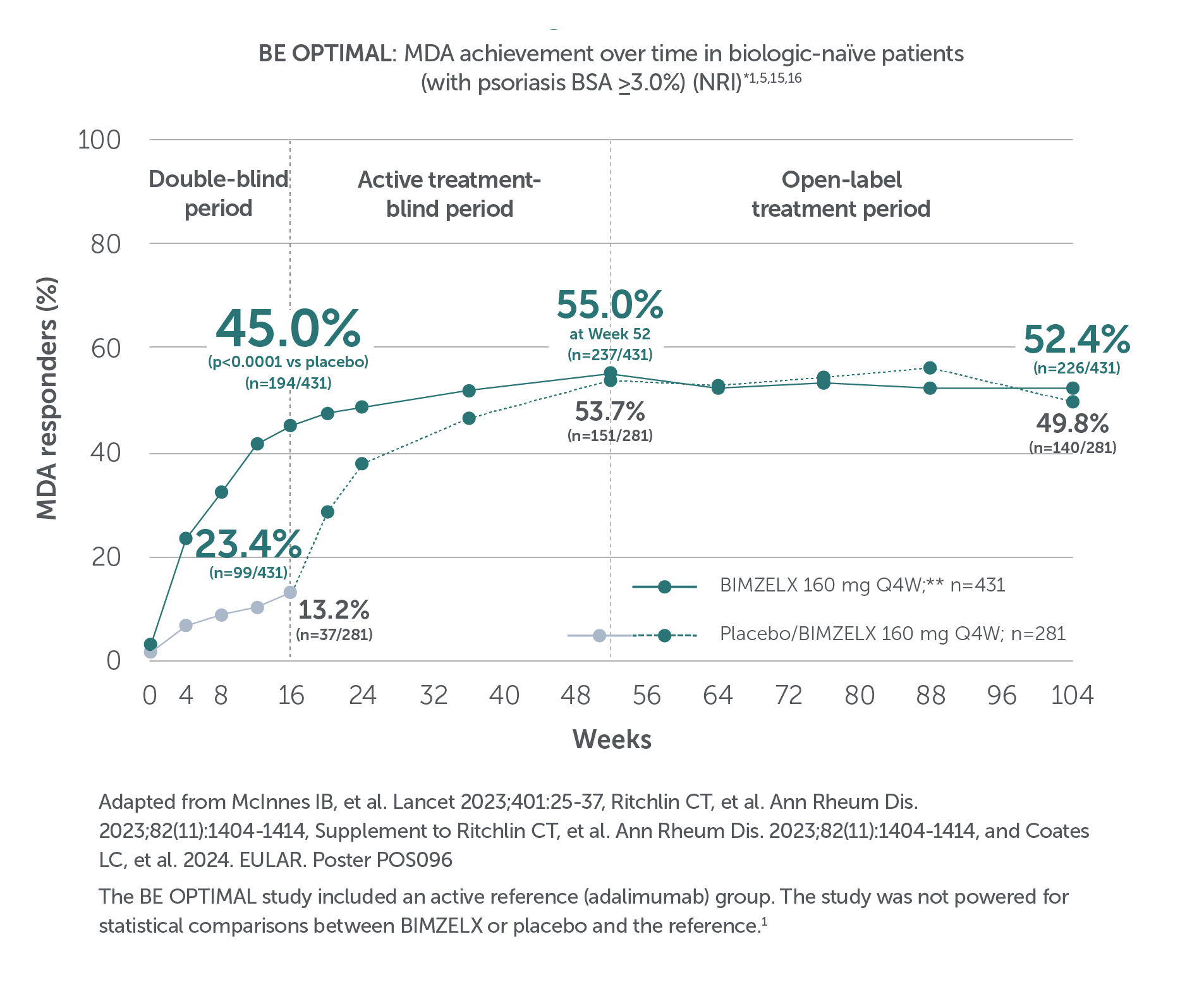
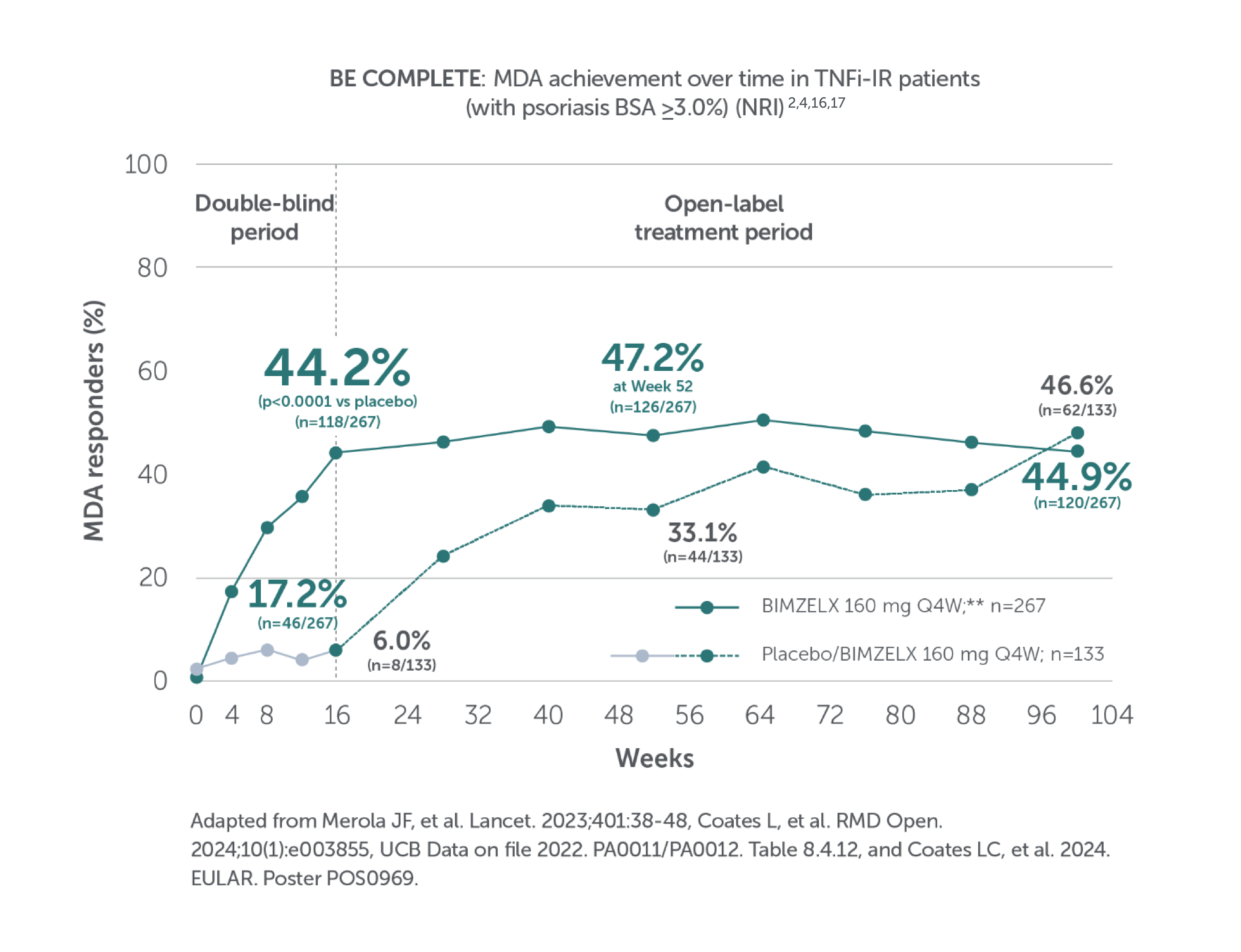
*In BE OPTIMAL, MDA was achieved by 23.4% (n=99/431) at Week 4 (vs 6.8% [n=19/281] with placebo),5 45.0% (n=194/431) at Week 16 (vs 13.2% [n=37/281] with placebo, p<0.0001), 55.0% (n=237/431) of patients in the BIMZELX treatment arm at Week 52,1,15 and 52.4% (n=226/431) of patients in the BIMZELX treatment arm at Week 104 (NRI analysis).16 In BE COMPLETE, MDA was achieved by 17.2% (n=46/267) at Week 4 (vs 4.5% [n=6/133] with placebo),17 44.2% (n=118/267) at Week 16 (vs 6.0% [n=8/133] with placebo, p<0.0001), 47.2% (n=126/267) of patients in the BIMZELX treatment arm at Week 522,4 and 44.9% (n=120/267) of patients in the BIMZELX treatment arm at Week 100 (NRI analysis).16 **BIMZELX is approved for Q4W/Q8W dosing with PsA in coexisting moderate-to-severe plaque psoriasis.3

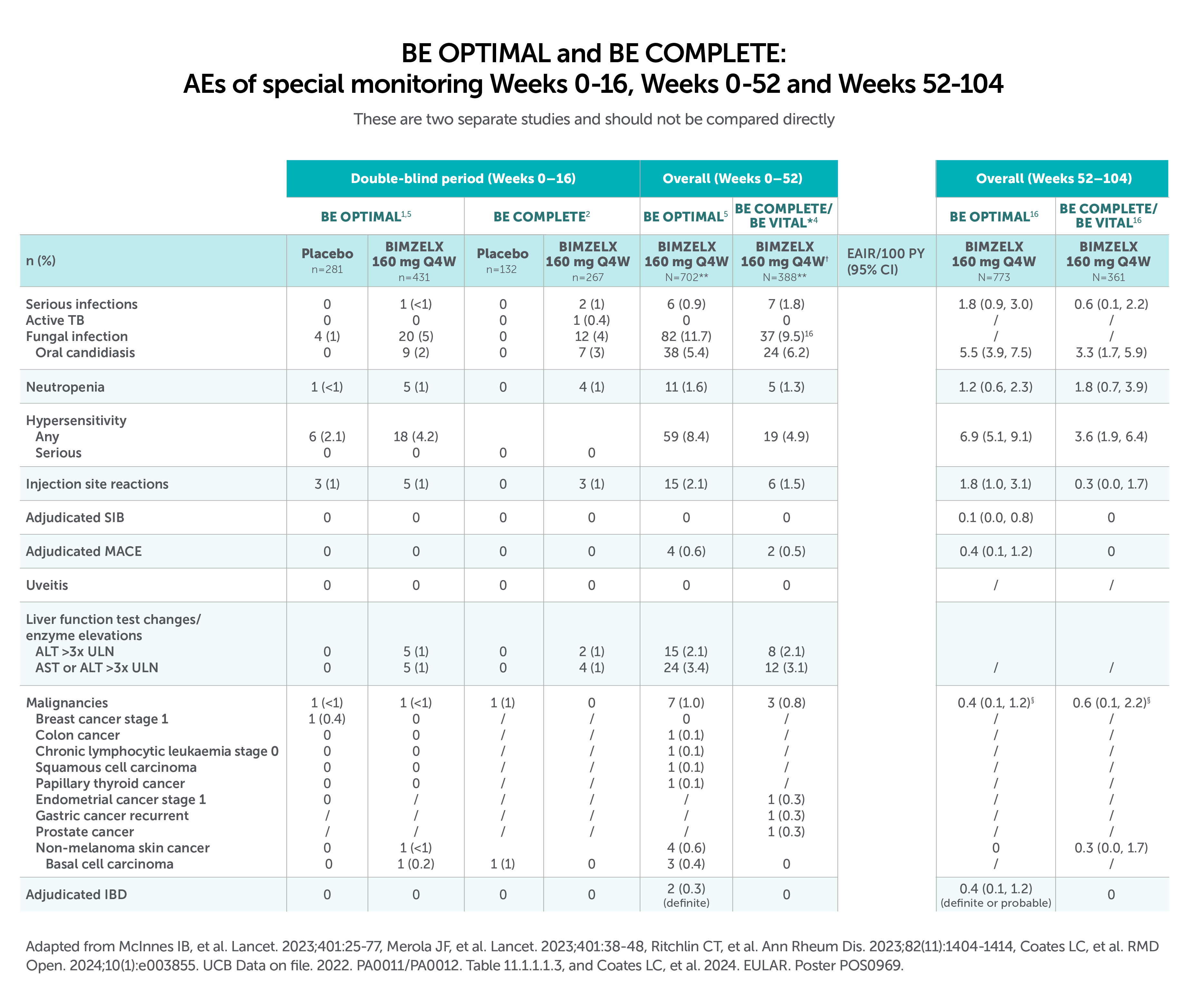
After Week 16, patients in BE OPTIMAL, BE COMPLETE, BE MOBILE 1 and BE MOBILE 2 were aware that they were receiving active treatment, which may have affected the results. *Week 52 data are from patients who completed BE COMPLETE and entered the BE VITAL open-label extension study.4 Week 52 data are from BE MOBILE 1 and BE MOBILE 2 and are the open-label maintenance phase of the studies.9 **Includes patients who switched from BIMZELX Q4W (events reports after the switch only).5,16 †One death occurred in a patient receiving BIMZELX due to a motorcycle accident.5 ‡One sudden death occurred in a patient with a history of cardiac events.4 ¥One death due to acute myocardial infarction, reported as unrelated to the study drug.16 §Malignancies excluding non-melanoma skin cancer.16
HOW TO USE
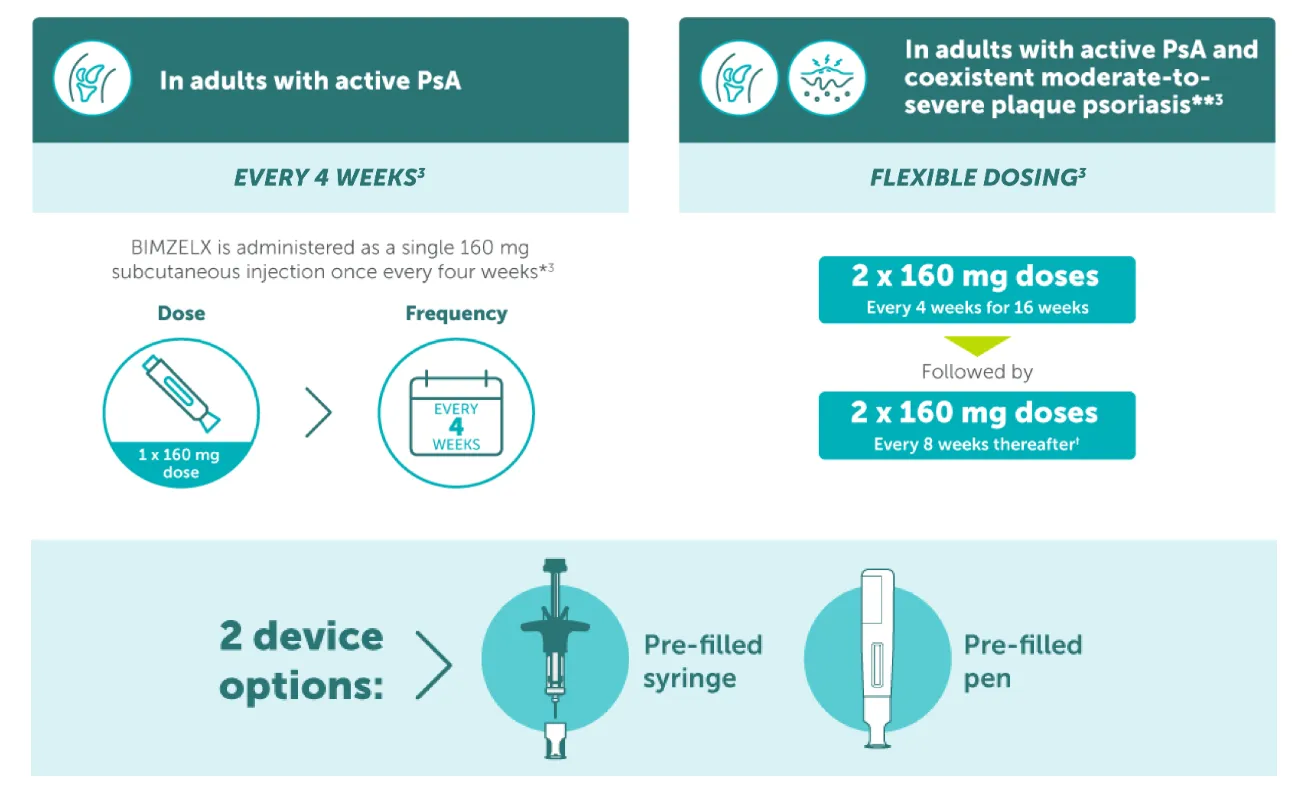
* The recommended dose for adult patients with active psoriatic arthritis is 160 mg (given as one subcutaneous injection of 160 mg) every 4 weeks. Consideration should be given to discontinuing treatment in patients who have shown no improvement by 16 weeks of treatment;3 **The recommended dose for adult patients with psoriatic arthritis and coexistent moderate-to-severe plaque psoriasis is the same as for plaque psoriasis, 320 mg (given as two subcutaneous injections of 160 mg each) at Week 0, 4, 8, 12, 16, and every 8 weeks thereafter. Consideration should be given to discontinuing treatment in patients who have shown no improvement by 16 weeks of treatment.3 †If a sufficient clinical responsed in the joints cannot be maintained after Week 16, a switch to 160 mg Q4W can be considered.3
Biologic-naïve patients with active PsA21
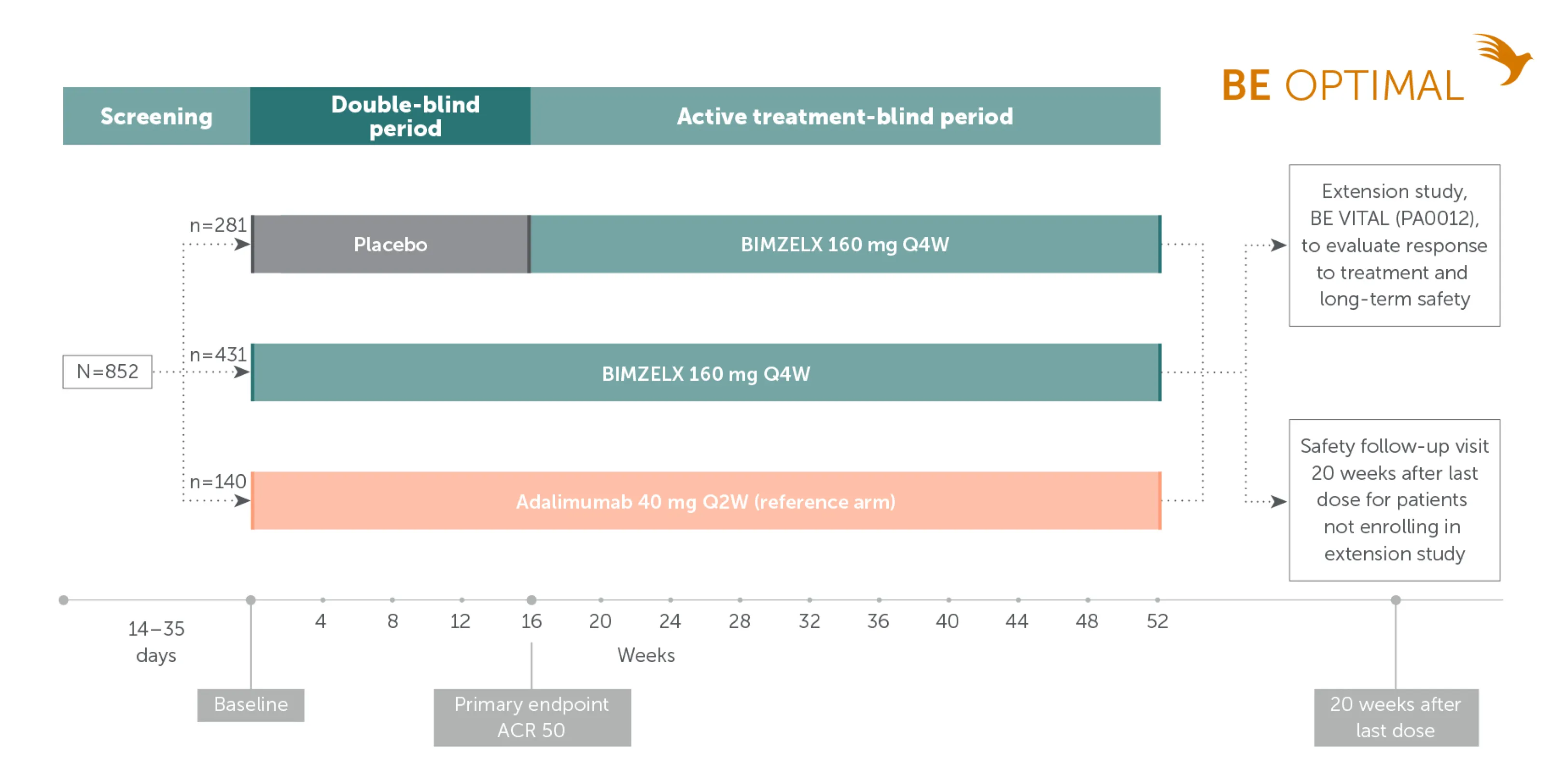
Adapted from McInnes IB, et al. Lancet. 2023;401:25-77. Supplementary appendix.
TNFi-inadequate responder patients with active PsA22
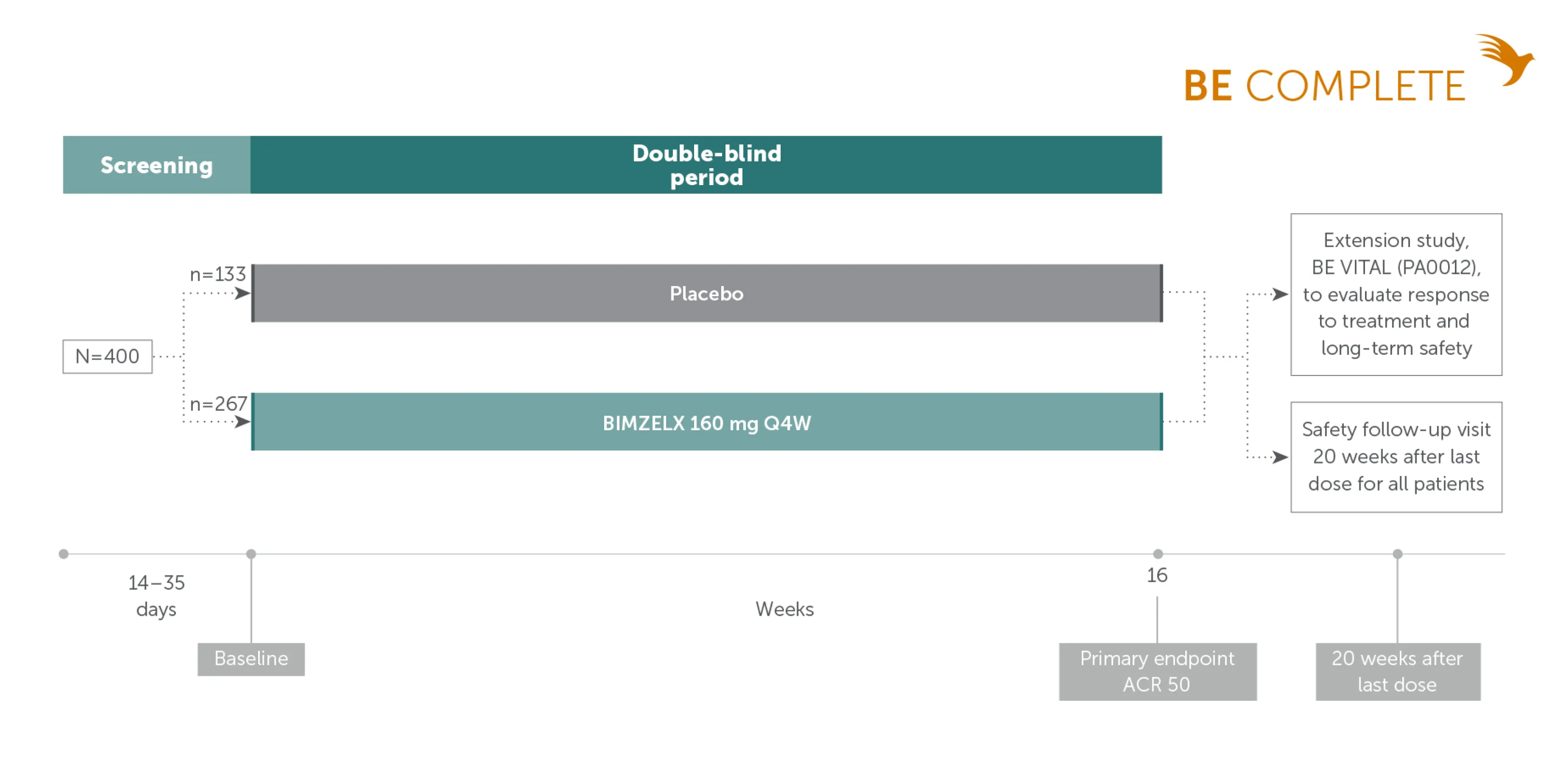
Adapted from Merola JF, et al. Lancet. 2023;401:38-48. Supplementary appendix.
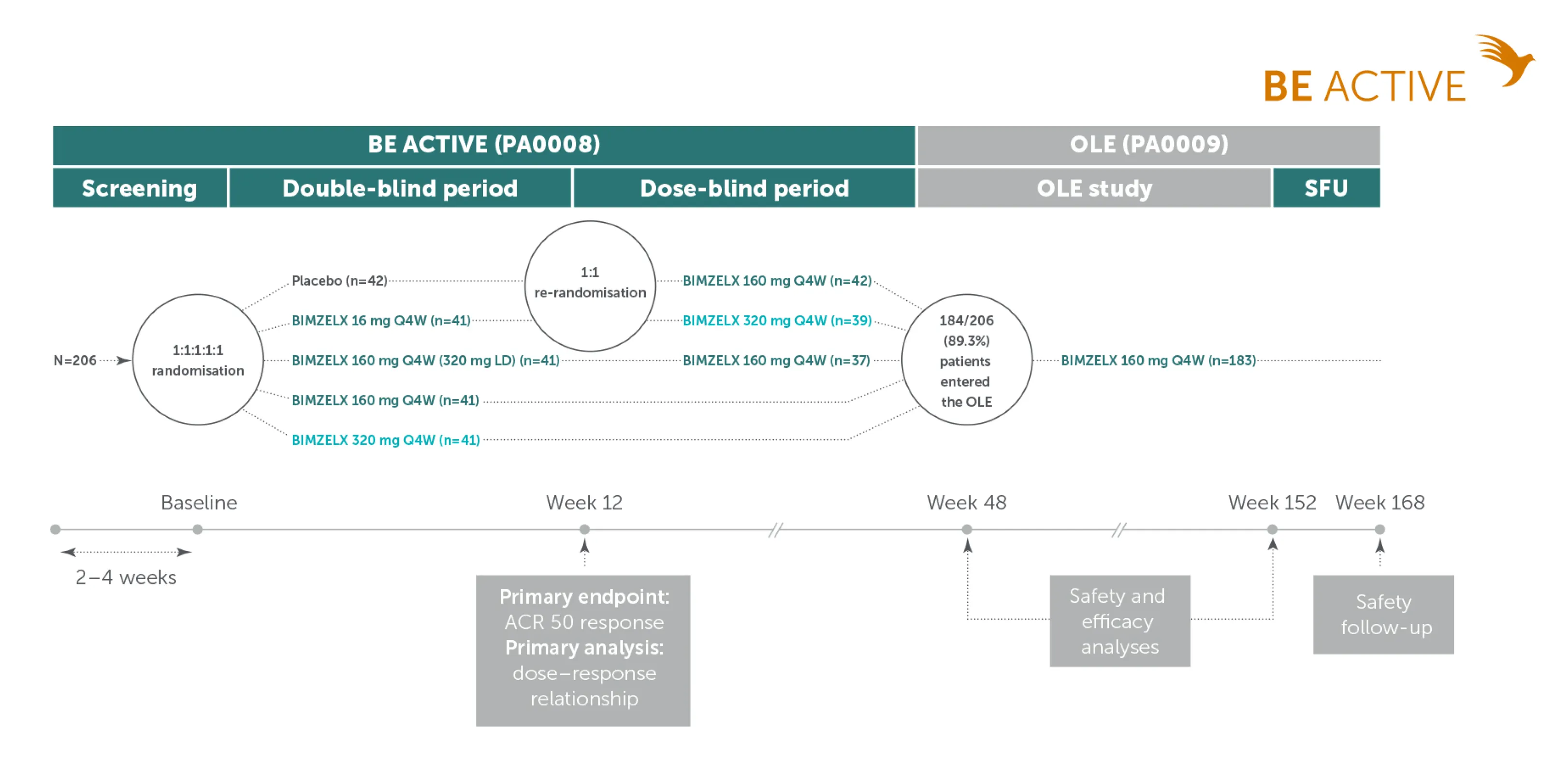
Adapted from Coates LC. et al. Arthritis Rheumatol. 2022;74:1959-1970. Supplementary appendix
IE-BK-2400114
Date of creation: November 2024