Image


▼This medicine is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare Professionals are asked to report any suspected adverse reactions. Adverse events should be reported. Reporting forms and information can be found at yellowcard.mhra.gov.uk for the UK and hpra.ie/homepage/about-us/report-an-issue for Ireland Or, via the MHRA Yellow Card App in the Google Play or Apple App Store. Adverse events should also be reported to UCB Pharma Limited at UCBCares.UK@ucb.com or 0800 2793177.
BIMZELX® (bimekizumab) is indicated for the treatment of: active PsA, alone or in combination with methotrexate, in adults who have had an inadequate response or who have been intolerant to one or more DMARDs; active nr-axSpA, in adults with objective signs of inflammation as indicated by elevated CRP and/or MRI, who have responded inadequately or are intolerant to NSAIDs; and active AS, in adults who have responded inadequately or are intolerant to conventional therapy.2
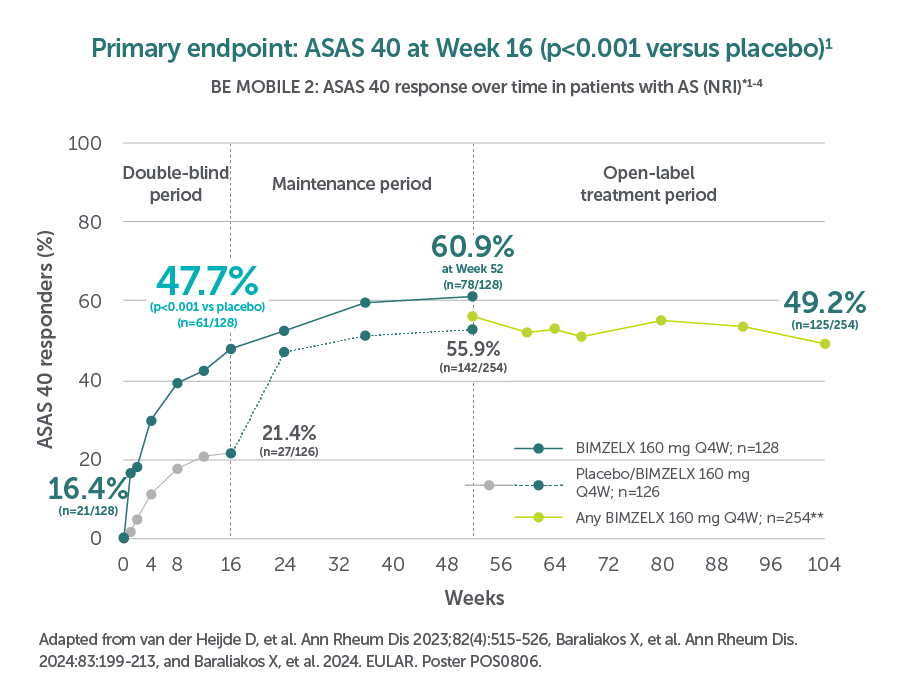
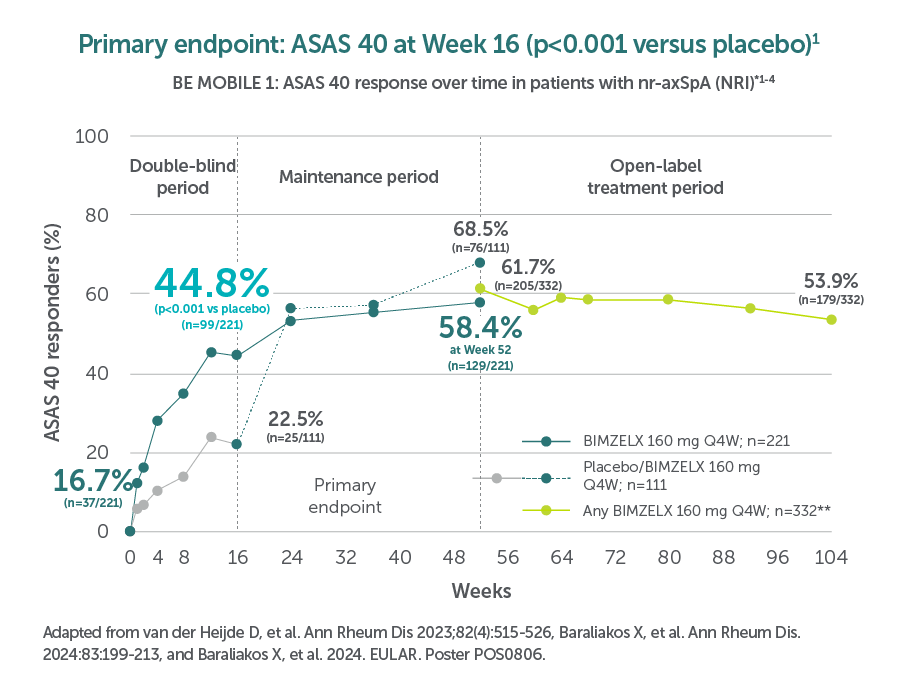
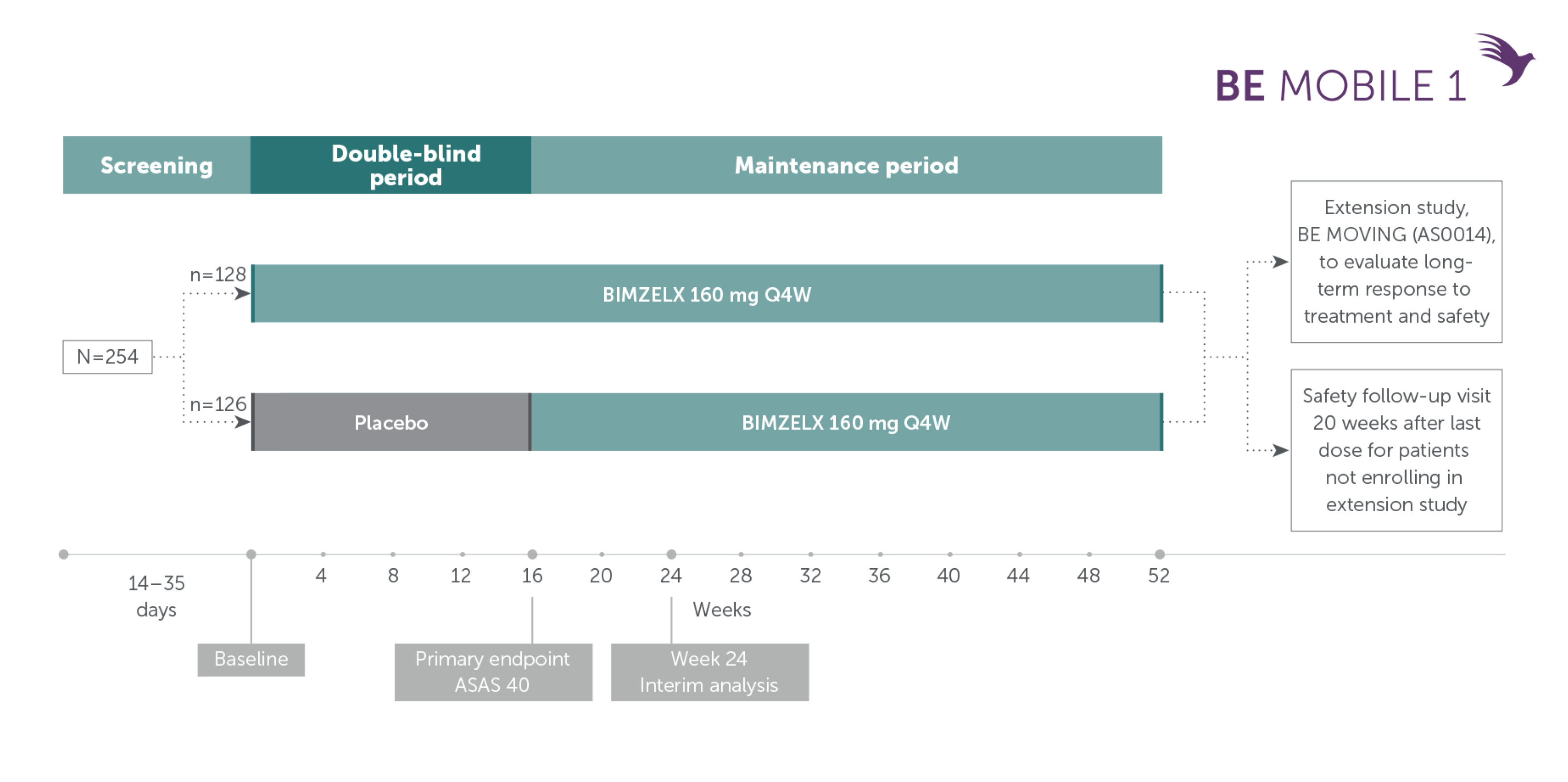
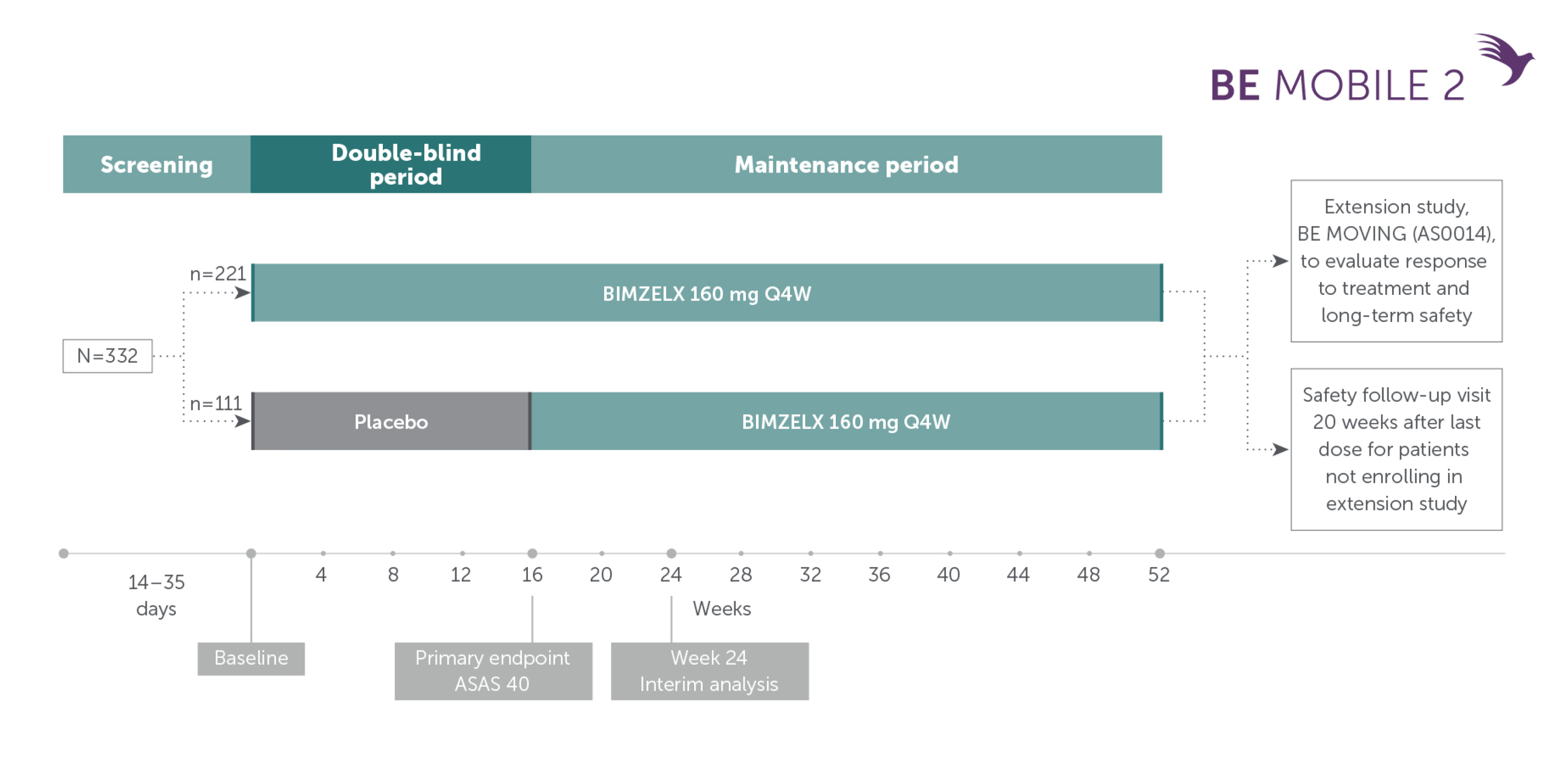
In two pivotal phase Ill trials, 47.7% (n=61/128) of patients with nr-axSpA and 44.8% (n=99/221) of patients with AS achieved the primary endpoint of ASAS 40 at Week 16 with BIMZELX (vs 21.4% [n=27/126] and 22.5% [n=25/111] with placebo, respectively; p<0.001 in both trials)1,2
After Week 16 patients in BE MOBILE 1 and BE MOBILE 2 were aware that they were receiving active treatment, which may have affected the results. 1
After Week 16 patients in BE MOBILE 1 and BE MOBILE 2 were aware that they were receiving active treatment, which may have affected the results. 1
*In BE MOBILE 1, ASAS 40 was achieved by 16.4% (n=21/128) with BIMZELX at Week 1 (vs 1.6% [n=2/126] with placebo),2,4 47.7% (n=61/128) at Week 16 (vs 21.4% [n=27/126] with placebo, p<0.001), and 60.9% (n=78/128) at Week 52 of patients with nr-axSpA in the BIMZELX treatment arm (NRI analysis).1,3 In the open-label treatment period, ASAS 40 was achieved by 49.2% (125/254) of patients with nr-axSpA receiving BIMZELX at Week 104 (NRI analysis). In BE MOBILE 2, ASAS 40 was achieved by 16.7% (n=37/221) with BIMZELX at Week 2 (vs 7.2% [n=8/111] with placebo),2,4 44.8% (n=99/221) at Week 16 (vs 22.5% [n=25/111] with placebo, p<0.001), and 58.4% (n=129/221) at Week 52 of patients with AS in the BIMZELX treatment arm (NRI analysis);3 In the open-label treatment period, ASAS 40 was achieved by 53.9% (179/332) of patients with AS receiving BIMZELX at Week 104 (NRI analysis).3 In BE MOBILE 1, 86.6% (n=220/254) of patients with nr-axSpA who completed 16 weeks of treatment remained on BIMZELX at Week 52. In BE MOBILE 2, 89.8% (n=298/332) of patients with AS who completed 16 weeks of treatment remained on BIMZELX at Week 52.3
**Includes patients originally randomised to placebo.3
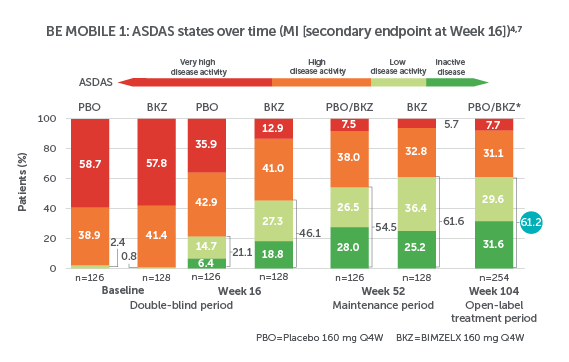
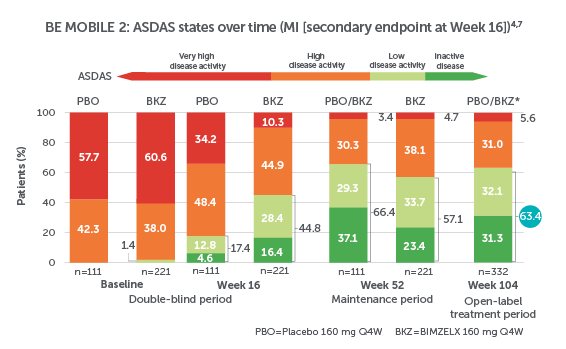
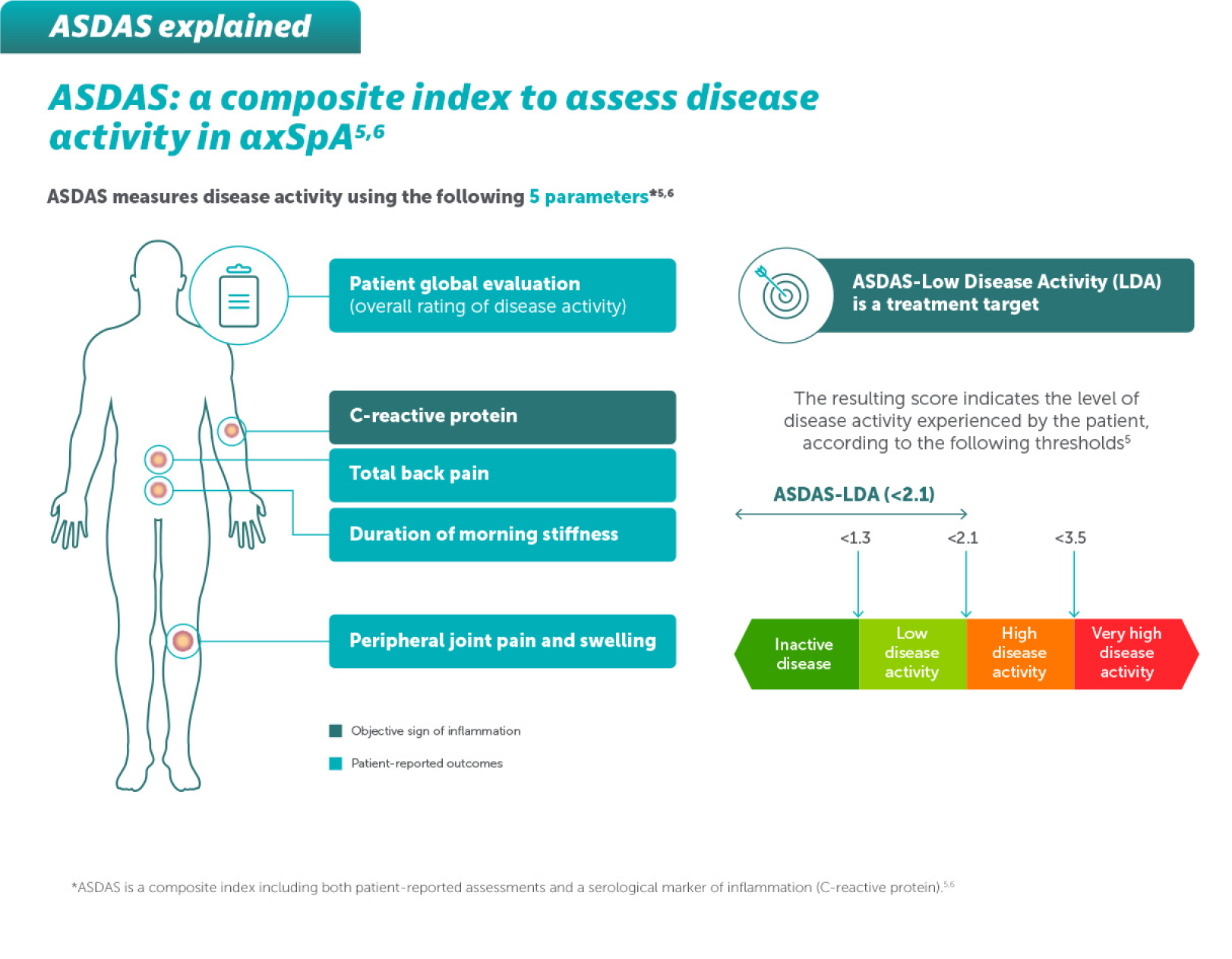
ASDAS measures disease activity using patient-reported outcomes and an objective sign of inflammation (CRP)*5,6
Adapted from Baraliakos X, et al. 2022. ACR Poster L14 and Baraliakos X, et al. 2024. EULAR. Poster POS0806.
After Week 16 all patients were aware that they were receiving active treatment, which may have affected the results.1
Adapted from Baraliakos X, et al. 2022. ACR Poster L14 and Baraliakos X, et al. 2024. EULAR. Poster POS0806.
After Week 16 all patients in BE MOBILE 1 & BE MOBILE 2 were aware that they were receiving active treatment, which may have affected the results.1
Week 104 data includes patients originally randomised to placebo.4
*ASDAS <2.1 values shown next to bars for Week 104 data are manually calculated from ASDAS state response rates.4 In BE MOBILE 1, ASDAS <2.1 was achieved by 61.2% (n=155/254) of patients with nr-axSpA at Week 104.4 In BE MOBILE 2, ASDAS <2.1 was achieved by 63.4% (n=210/332) of patients with AS at Week 104.4 ASDAS-MI response at Weeks 24 and 52 was an exploratory endpoint.1
57.7% (30/52) of patients with nr-axSpA and 61.3%) (19/31) of patients with AS achieved MRI remission at Weeks 104 (OC)*
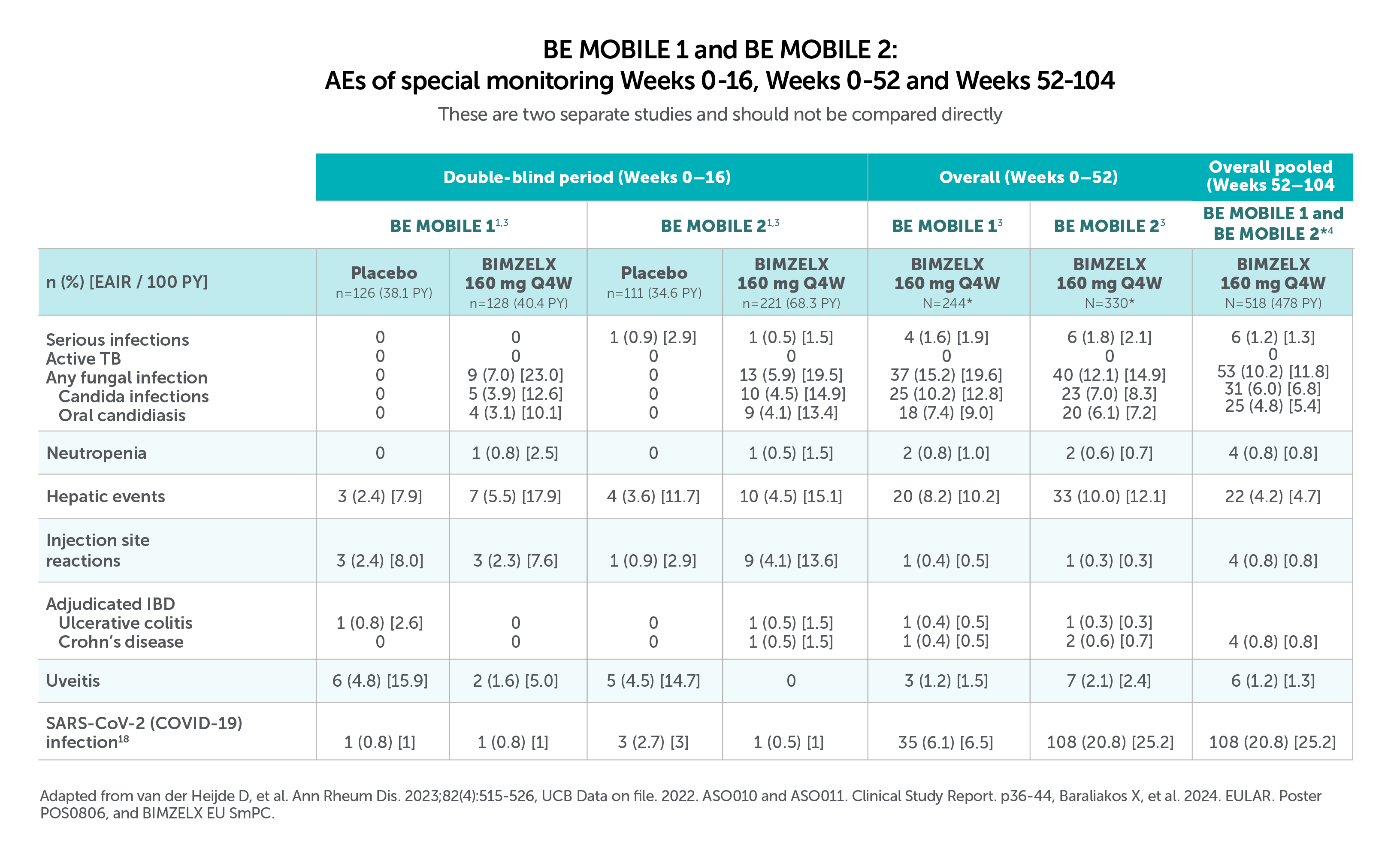
These are two separate studies and should not be compared directly
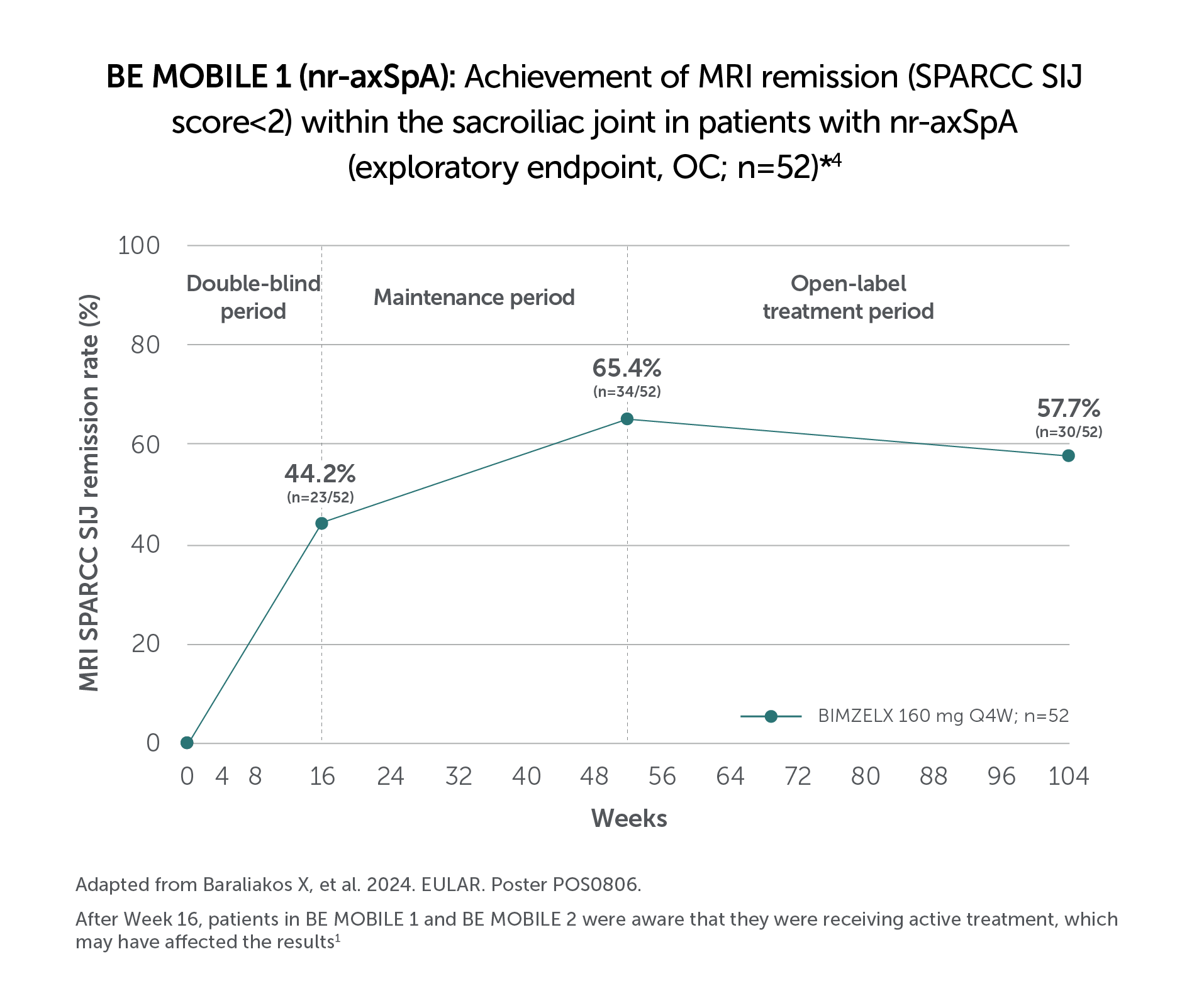
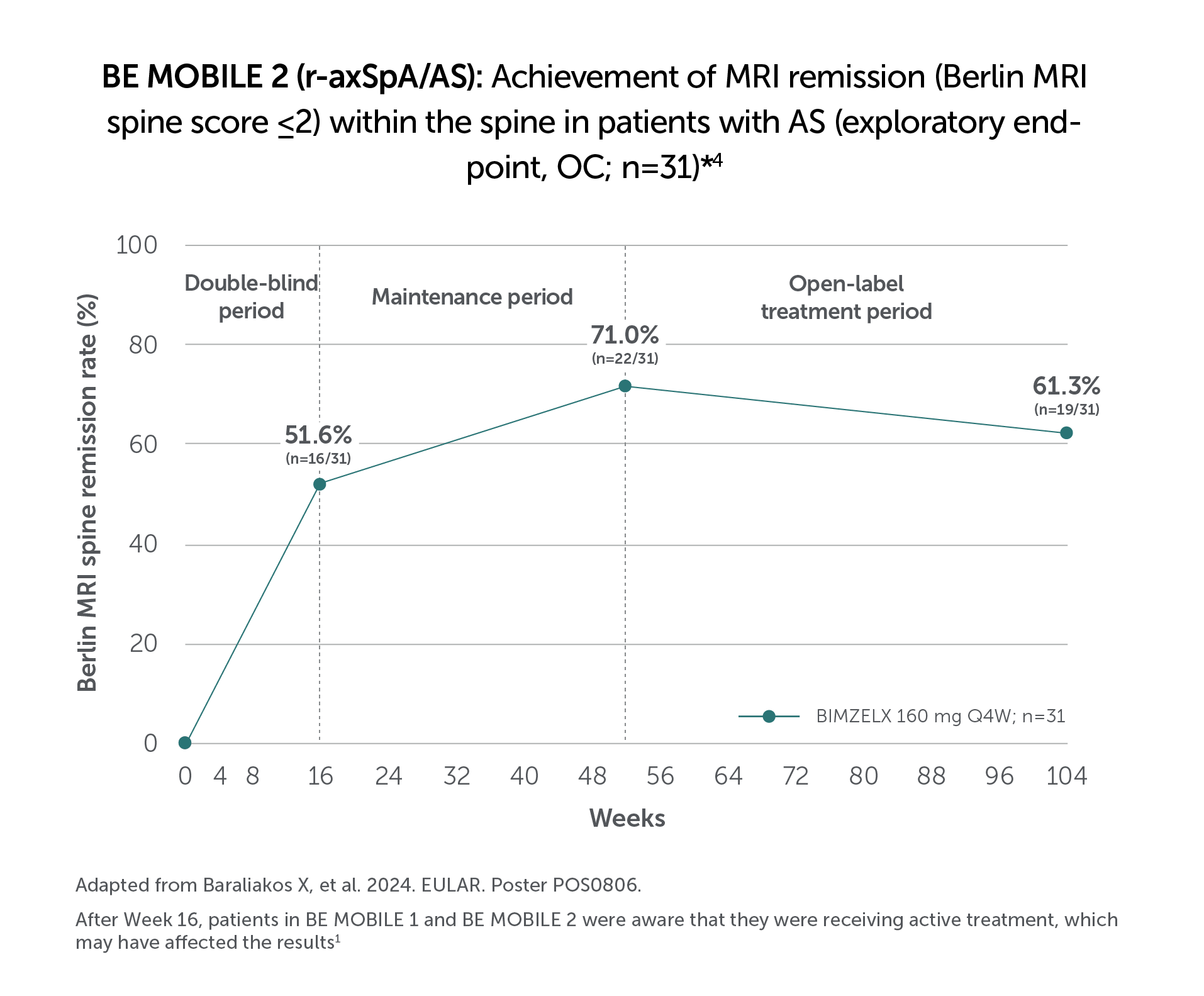
*MRI sub-study enrolling patients receiving BIMZELX with baseline MRI SIJ SPARCC ≥2 (nr-axSpA; n=52) or baseline Berlin MRI spine score >2 (AS; n=31) MRI remission is defined as MRI SIJ SPARCC <2 or Berlin MRI spine score ≤2.4
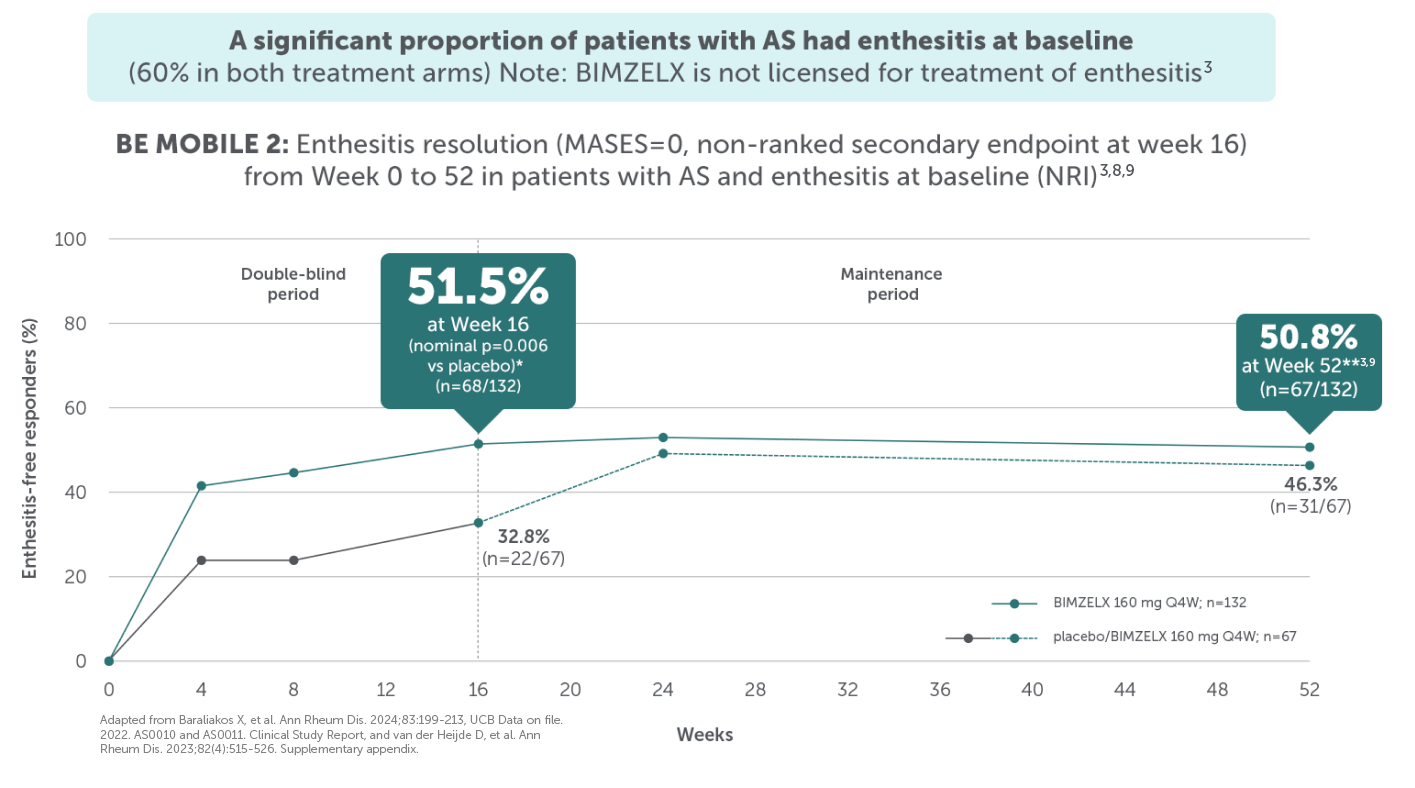
After Week 16 patients in BE MOBILE 1 and BE MOBILE 2 were aware that they were receiving active treatment, which may have affected the results.1
After Week 16 patients in BE MOBILE 1 and BE MOBILE 2 were aware that they were receiving active treatment, which may have affected the results. 1
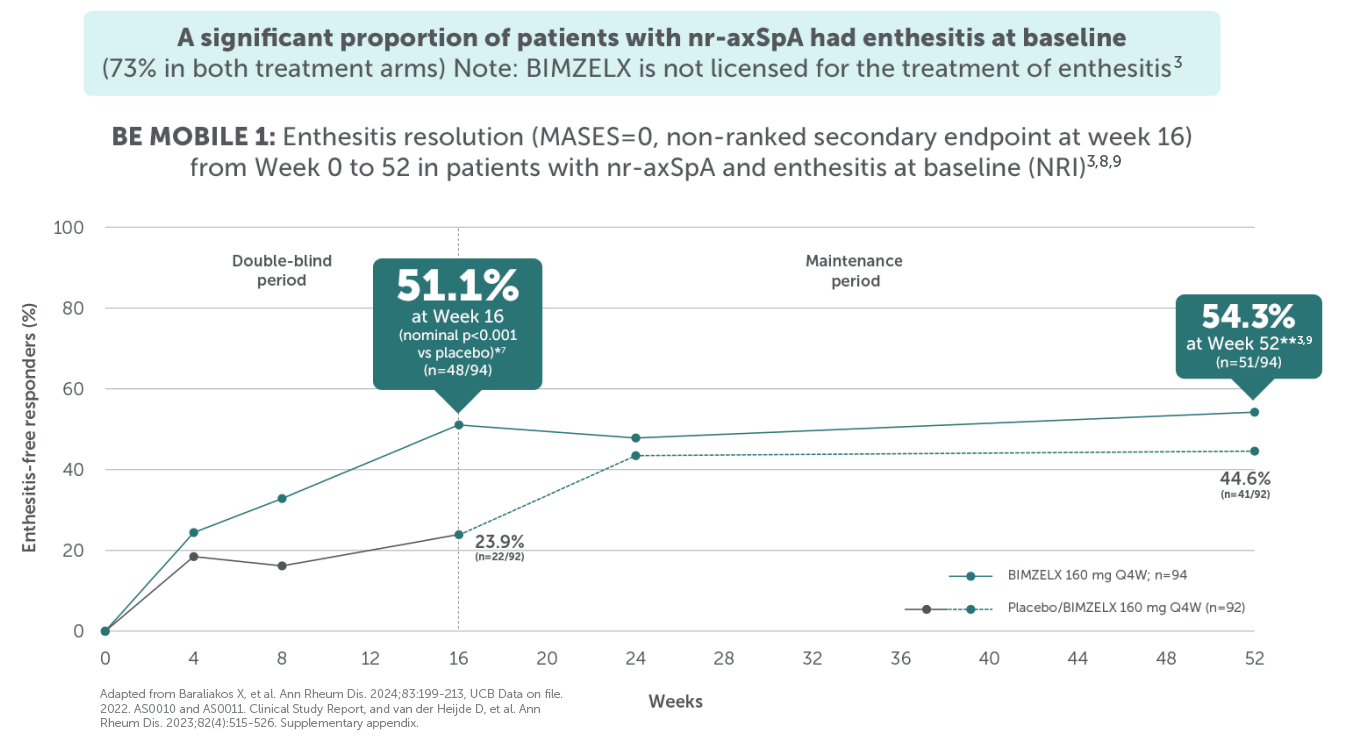
*In BE MOBILE 1, complete resolution of enthesitis, measured via MASES=0, was achieved by 51.1% (n=48/94) in the BIMZELX treatment arm versus 23.9% (n=22/92) in the placebo arm at Week 16, nominal p<0.001 (NRI analysis).8,9 In BE MOBILE 2, complete resolution of enthesitis, measured via MASES=0, was achieved by 51.5% (n=68/132) in the BIMZELX treatment arm versus 32.8% (n=22/67) in the placebo arm at Week 16, nominal p<0.001 (NRI analysis);8,9 **In BE MOBILE 1 and BE MOBILE 2, complete resolution of enthesitis (MASES=0) was achieved by 54.3% (n=51/94) of patients with nr-axSpA and 50.8% (n=67/132) of patients with AS at Week 52.3
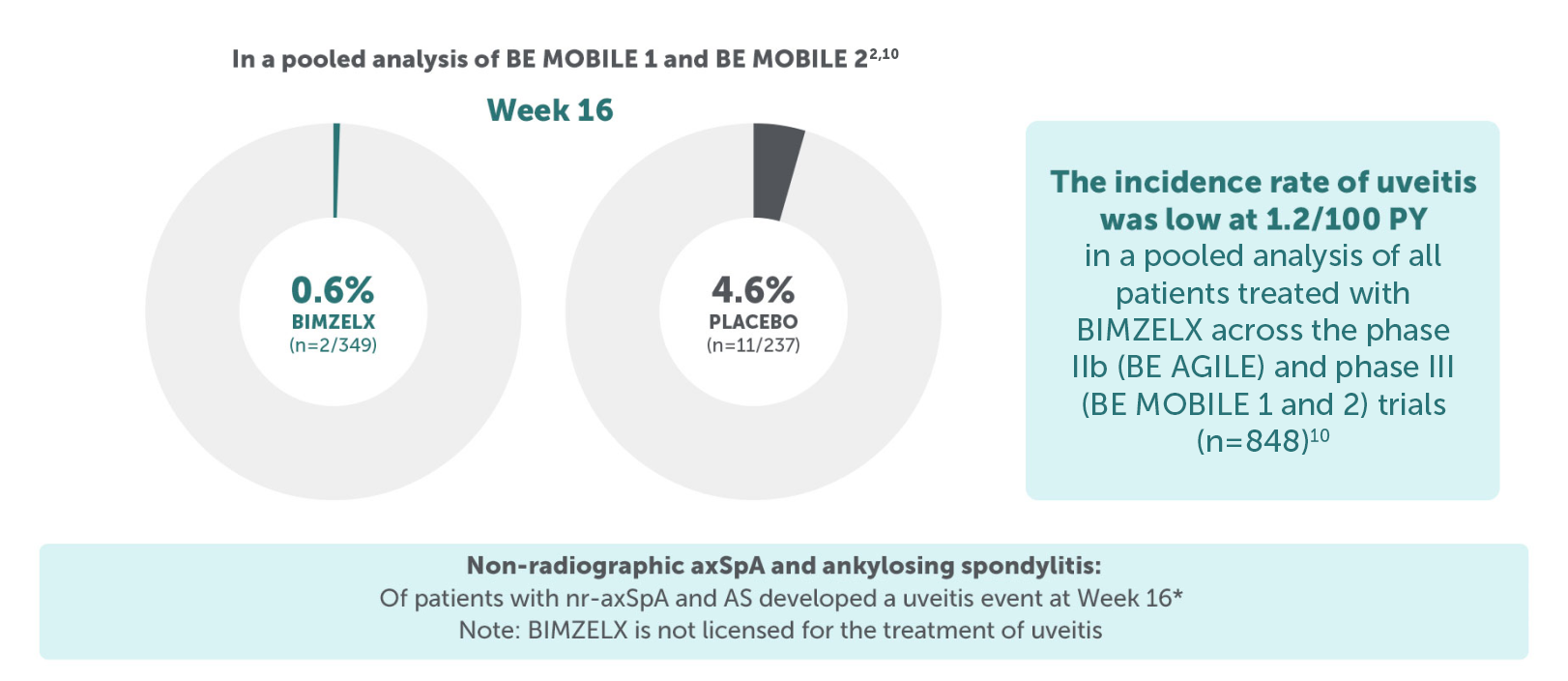
*Of 349 patients randomised to BIMZELX treatment across BE MOBILE 1 and BE MOBILE 2, 14.9% (n=52) had a history of uveitis at baseline (pooled data).1
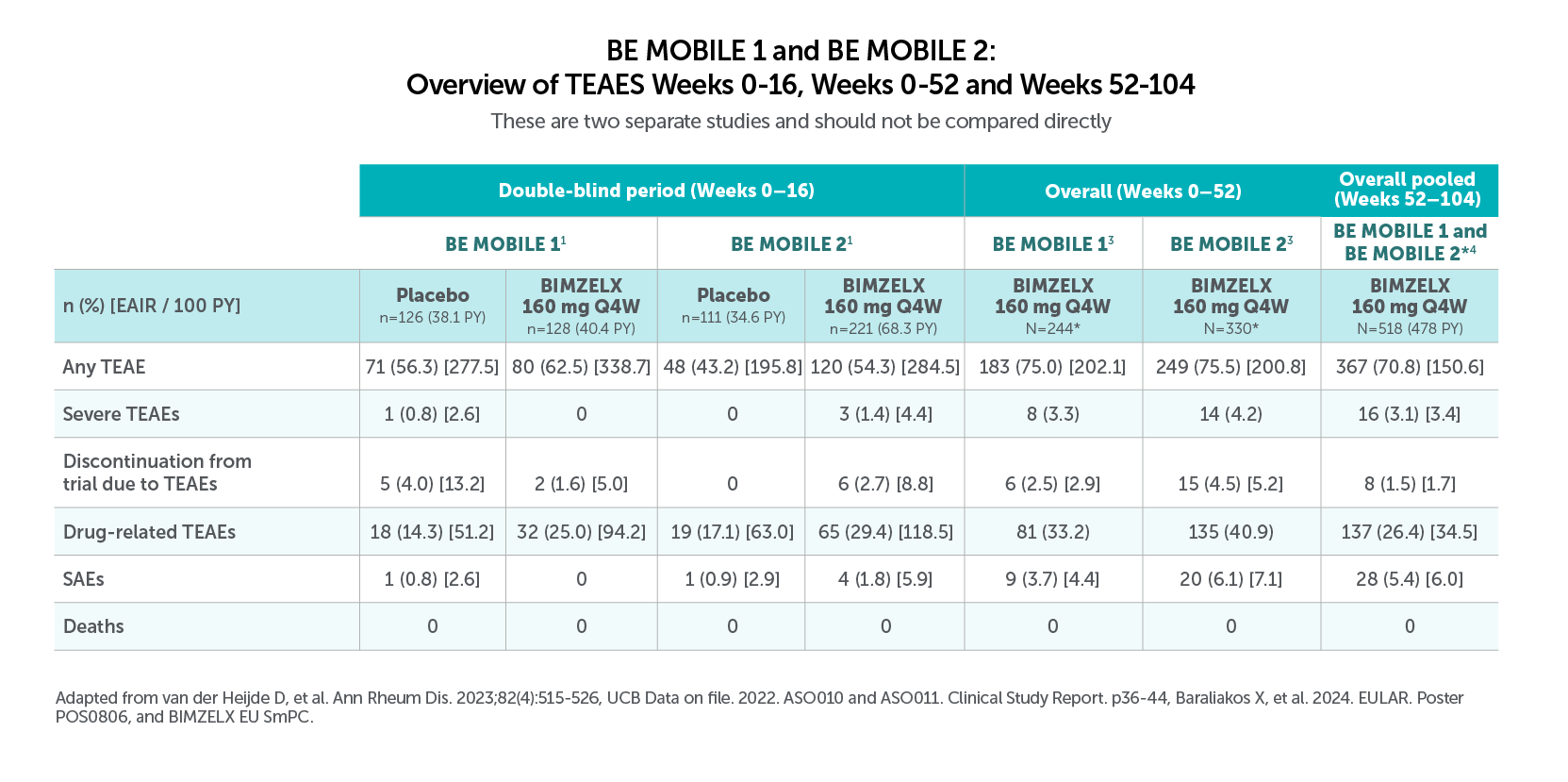
Most common TEAES (>5.0% in BE MOBILE 1 and BE MOBILE 2) with BIMZELX across 52 weeks were:
• Nasopharyngitis (12.3%, n=30/244, and 9.1%, n=30/330), oral candidiasis (7.4%, n=18/244, and 6.1%, n=20/330), and URTIS (9.4%, n=23/244, and 6.4%, n=21/330) in BE MOBILE 1 and BE MOBILE 2, respectively3
Most frequent TEAEs to Week 104 by preferred term (EAIR/100 PY) were COVID-19 Infection (13.2), nasopharyngitis (10.2), and upper respiratory tract infection (6.0),22Most frequent TEAEs to Week 104 by preferred term (EAIR/100 PY) were COVID-19 infection (13.2), nasopharayngitis (10.2), and upper respiratory tract infection (6.0).4
*Patient population is pooled and includes patients from both BE MOBILE 1 and BE MOBILE 2 who received a dose of BIMZELX, including those originally randomised to placebo, events are reported after switch only.4
Most common TEAES (>5.0% in BE MOBILE 1 and BE MOBILE 2) with BIMZELX across 52 weeks were:
• Nasopharyngitis (12.3%, n=30/244, and 9.1%, n=30/330), oral candidiasis (7.4%, n=18/244, and 6.1%, n=20/330), and URTIS (9.4%, n=23/244, and 6.4%, n=21/330) in BE MOBILE 1 and BE MOBILE 2, respectively3
Most frequent TEAEs to Week 104 by preferred term (EAIR/100 PY) were COVID-19 Infection (13.2), nasopharyngitis (10.2), and upper respiratory tract infection (6.0),22Most frequent TEAEs to Week 104 by preferred term (EAIR/100 PY) were COVID-19 infection (13.2), nasopharayngitis (10.2), and upper respiratory tract infection (6.0).4
*Patient population is pooled and includes patients from both BE MOBILE 1 and BE MOBILE 2 who received a dose of BIMZELX, including those originally randomised to placebo, events are reported after switch only.4
BIMZELX is administered as a single 160 mg subcutaneous injection once every 4 weeks*2
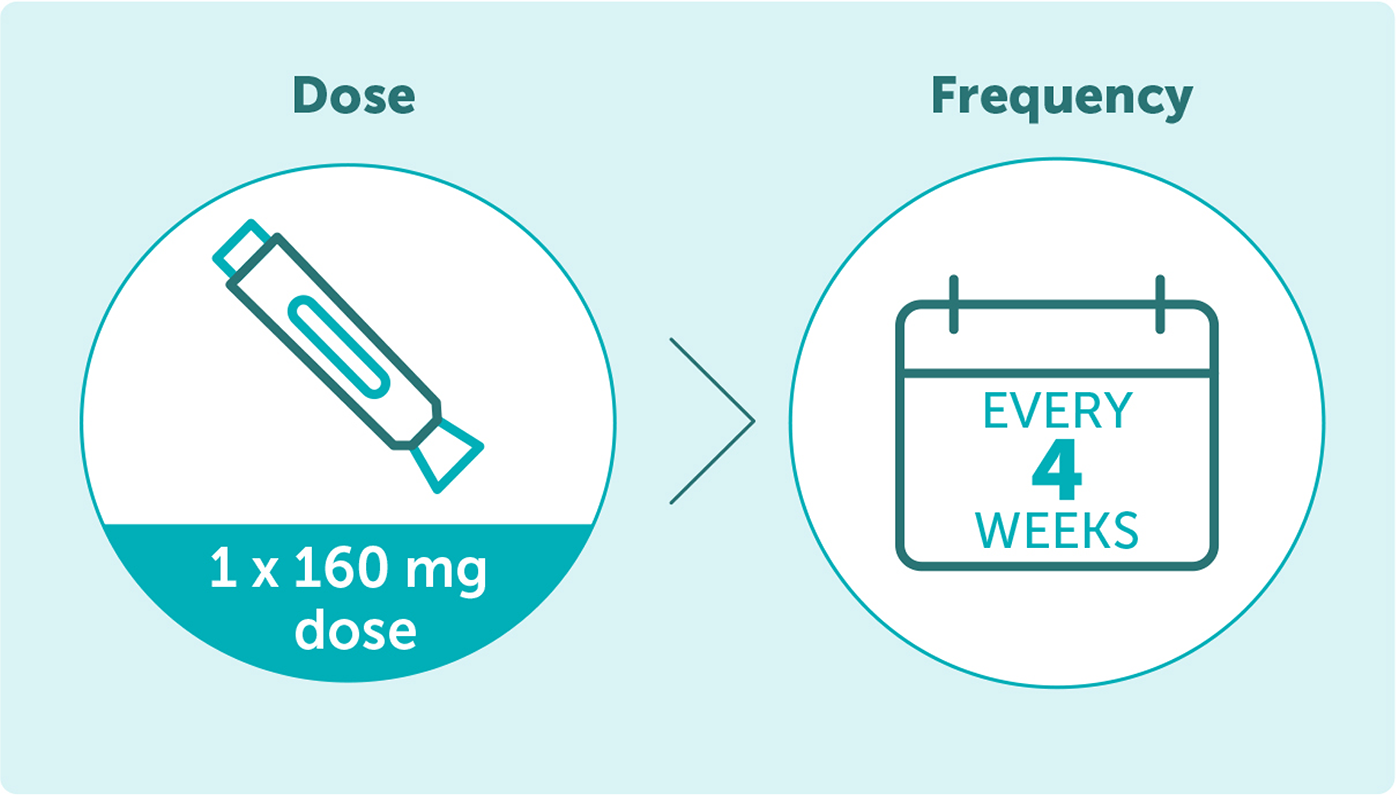
*The recommended dose for adult patients with axial spondyloarthritis is 160 mg (given as one subcutaneous injection) every four weeks. Consideration should be given to discontinuing treatment in patients who have shown no improvement by 16 weeks of treatment.2
Adapted from van der Heijde D, et al. Ann Rheum Dis. 2023; 82(4):515-526. Supplementary appendix.
Adapted from van der Heijde D, et al. Ann Rheum Dis. 2023; 82(4):515-526. Supplementary appendix.
Adapted from Baraliakos X, et al. Arthritis Rheumatol. 2022; 71(q12): 1943-58. Supplementary Appendix.
IE-BK-2400125
Date of creation: September 2024